




Research
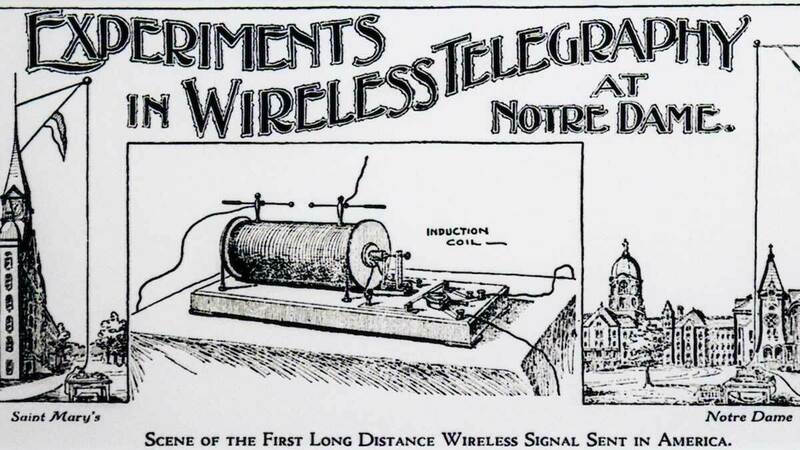
Notre Dame celebrates 125 years of wireless innovation and education
The University of Notre Dame is celebrating 125 years of wireless research, education and innovation with a modern re-enactment of one of the first long-range wireless transmissions conducted in the United States and a full-day symposium of panels and…




